 pic.PNG)
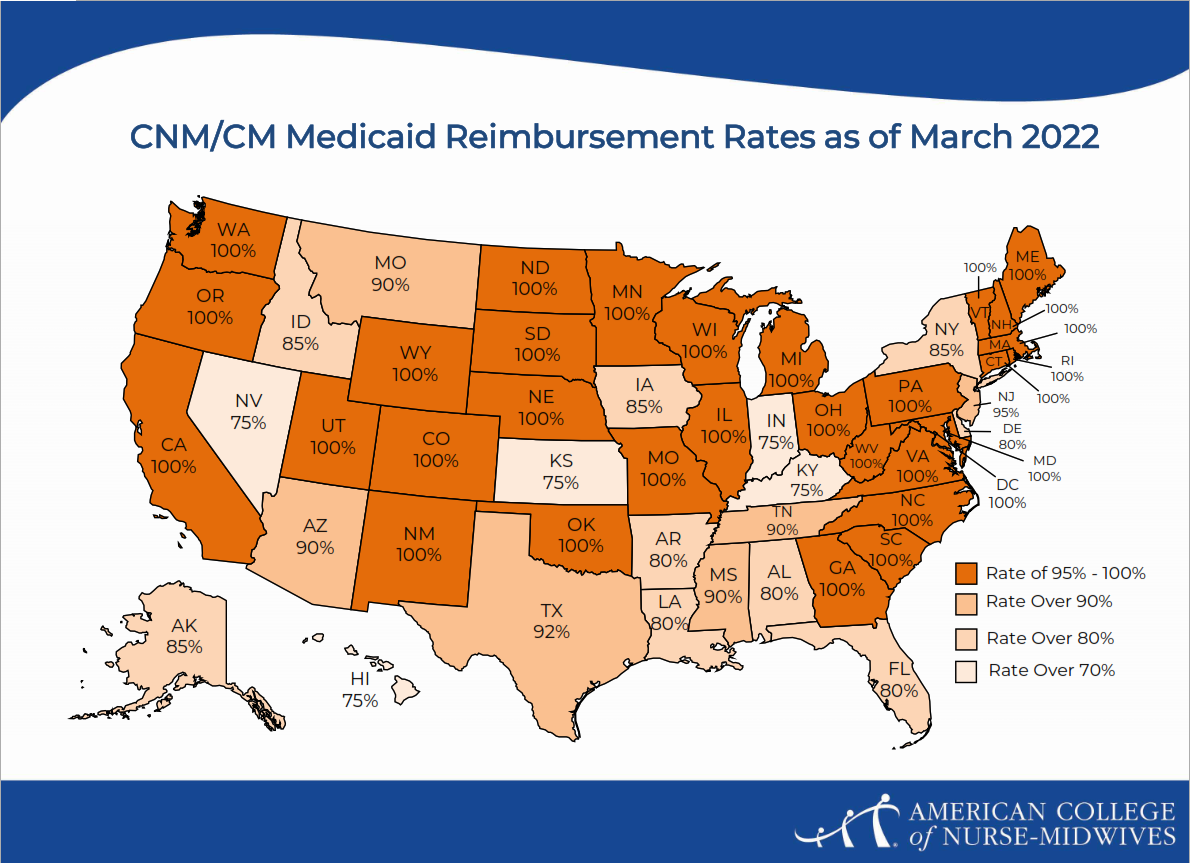
The first map shows how much physicians are reimbursed by Medicaid as a percentage of the rates set by Medicare/Centers for Medicare & Medicaid Services. The second map show what percentage of that physician rate is paid to CNMs and CMs. For example: in Texas, the Medicaid physician rate is 66% of the rate set by Medicare. CNMs in Texas would get 92% of that reduced rate. Not every state reimburses CNMs and CMs at 100% of the physician fee schedule. It’s clear that a reduced rate of a reduced rate can restrict access for patients seeking midwifery care. Also, CNMs and CMs may not be listed in the participating providers list for insurers. So when people think that their insurance doesn’t cover midwifery care, they may not get a midwife when they want one. Also, employers may not be inclined to hire CNMs or CMs if they are reimbursed at a rate lower than the physicians’ rate for the same services/codes/charges. Or practice/health system billers may bill “incident to” under the physician’s name for the higher rate and the CNMs’ or CMs’ work is invisible.
Competitive and equitable rates of reimbursement will support the financial viability of midwifery care and birth centers, which we know will improve health outcomes for pregnant people and their infants. This is a structural reform that will help improve access to midwifery-led models of care and make health equity a reality.
Sample reimbursement equity bill language:
From Connecticut General Assembly 2021
AN ACT CONCERNING MEDICAID PROVIDERS.
Be it enacted by the Senate and House of Representatives in General Assembly convened:
1 Section 1. Section 17b-28e of the general statutes is amended by
2 adding subsection (d) as follows (Effective from passage):
3 (NEW) (d) Not later than October 1, 2021, the Commissioner of Social
4 Services shall amend the Medicaid state plan to include services
5 provided by acupuncturists licensed pursuant to section 20-206bb and
6 chiropractors licensed pursuant to section 20-27 as optional services
7 under the Medicaid program.
8 Sec. 2. Section 17b-280c of the general statutes is repealed and the
9 following is substituted in lieu thereof (Effective July 1, 2021):
10 (a) For purposes of this section: (1) "Methadone maintenance" means
11 a chemical maintenance program under which an addiction to one drug,
12 including, but not limited to, heroin, is treated with the drug methadone
13 in a weekly program that includes on and off-site methadone
14 administration, drug testing and counseling; and (2) "chemical
15 maintenance provider" means a provider certified and licensed by the
16 federal Substance Abuse and Mental Health Services Administration
17 and the state Department of Public Health who meets all federal and
18 state requirements, including, but not limited to, requirements specific
19 to the provision of chemical maintenance services.
20 (b) The Commissioner of Social Services shall amend the Medicaid
21 state plan to provide a minimum weekly reimbursement rate of eighty-
22 eight dollars and fifty-two cents to a chemical maintenance provider for
23 methadone maintenance treatment of a Medicaid beneficiary, provided
24 no such provider receiving a higher rate shall have such rate reduced to
25 the minimum as a result of the implementation of a new minimum
26 reimbursement rate.
27 [(c) Notwithstanding subsection (b) of this section, on or after July 1,
28 2020, any reimbursement to a chemical maintenance provider for
29 methadone maintenance treatment shall be contingent upon meeting
30 certain performance measures as determined by the commissioner. Such
31 performance measures shall be developed in consultation with the
32 Department of Mental Health and Addiction Services and chemical
33 maintenance providers. Initial performance measures shall be
34 developed by September 30, 2019, including the means by which such
35 measures shall be evaluated. The initial evaluation period shall be based
36 on the claims data for the quarter ending March 31, 2020. The
37 performance measures and thresholds may be adjusted after the initial
38 evaluation period. Failure to meet department-identified standards on
39 performance measures shall result in a rate reduction of (1) up to five
40 per cent for the quarters ending September 30, 2020, and December 31,
41 2020, and (2) up to ten per cent beginning January 1, 2021. No provider
42 shall receive a rate decrease under this subsection that is more than a ten
43 per cent decrease annually.]
44 [(d)] (c) The Commissioner of Social Services, pursuant to section 17b-
45 10, may implement policies and procedures to administer the provisions
46 of this section while in the process of adopting such policies and
47 procedures in regulation form, provided the commissioner [prints]
48 posts notice of the intent to adopt the regulations on the department's
49 Internet web site and the eRegulations System not later than twenty
50 days after the date of implementation. Such policies and procedures
51 shall be valid until the time final regulations are adopted.
52 Sec. 3. (NEW) (Effective from passage) The Commissioner of Social
LCO {\\PRDFS1\SCOUSERS\FORZANOF\WS\2021SB-00764- 2 of 3 R02-SB.docx }
Substitute Bill No. 764
53 Services shall adjust rates of reimbursement under the Medicaid
54 program so that (1) a nurse-midwife licensed pursuant to chapter 377 of
55 the general statutes receives the same rate as an obstetrician-
56 gynecologist licensed pursuant to chapter 370 of the general statutes for
57 performing the same medical service or procedure, and (2) a podiatrist
58 licensed pursuant to chapter 375 of the general statutes receives the
59 same rate as a physician licensed pursuant to chapter 370 of the general
60 statutes for performing the same medical service or procedure. The
61 commissioner shall seek federal approval to amend the Medicaid state
62 plan, if necessary, to adjust rates of reimbursement in accordance with
63 this section.
64 Sec. 4. (NEW) (Effective July 1, 2021) The Commissioner of Social
65 Services shall amend the Medicaid state plan to integrate services
66 provided by peer support specialists into care teams funded under the
67 medical assistance program and provide Medicaid reimbursement to
68 such specialists for such services. For purposes of this section, "peer
69 support services" means a recovery-focused behavioral health service
70 that allows an individual the opportunity to learn to manage his or her
71 recovery with help from a peer support specialist who may have
72 experience recovering from mental illness or substance use disorder.
|
This act shall take effect as follows and shall amend the following sections: |
||
|
Section 1 |
from passage |
17b-28e |
|
Sec. 2 |
July 1, 2021 |
17b-280c |
|
Sec. 3 |
from passage |
New section |
|
Sec. 4 |
July 1, 2021 |
New section |
Statement of Purpose:
To add acupuncture and chiropractor services to those covered under Medicaid, adjust the Medicaid payment methodology for methadone maintenance providers, achieve Medicaid payment parity for nurse-midwives and podiatrists performing the same services as physicians, and provide Medicaid reimbursement to peer support specialists.
[Proposed deletions are enclosed in brackets. Proposed additions are indicated by underline, except that when the entire text of a bill or resolution or a section of a bill or resolution is new, it is not underlined.]
References
Attanasio, L. B., Alarid-Escudero, F., & Kozhimannil, K. B. (2019). Midwife-led care and
obstetrician-led care for low-risk pregnancies: A cost comparison. Birth, 47(1), 57-66. https://doi.org/10.1111/birt.1...
Courtot, B., Hill, I., Cross-Barnet, C., & Markell, J. (2020). Midwifery and birth centers under
state medicaid programs: Current limits to beneficiary access to a high-value model of
care. The Milbank Quarterly, 98(4), 1091-1113. https://doi.org/10.1111/1468-0...
Dudley, B. Promoting midwifery and high value care in Medi-Cal. Pacific Business Group on Health.
Kozhimannil, K. B., Henning-Smith, C., Hung, P., Casey, M. M., & Prasad, S. (2016). Ensuring
access to high-quality maternity care in rural America. Women’s Health Issues, 26(3),
247-250. https://doi.org/10.1016/j.whi....
Kozhimannil, K. B., Attanasio, L., Alarid-Escudero, F. (2019). More midwife-led care could
generate cost savings and health improvements. University of Minnesota School of Public Health.
Institute for Medicaid Innovation. (2020). Improving maternal health access, coverage, and
outcomes in Medicaid.
Medicaid and CHIP Payment and Access Commission. (2020). Inventory of state-level Medicaid
policies, programs, and initiatives to improve maternity care and outcomes.
National Academies of Sciences, Engineering, and Medicine. (2020). Birth settings in America:
Outcomes, quality, access, and choice. The National Academies Press.
https://doi.org/10.17226/25636
Pacific Business Group on Health. (2016). Barriers to Certified Nurse-Midwife (CNM) Care in California.
Pierce-Wrobel, C., Green, K., & Zephyrin, L. (2020, June 30). Attaining equitable high-value
maternity care. The Commonwealth Fund. https://doi.org/10.26099/hzvj-...
Ranji, U., Gomez, I., & Salganicoff, A. (2021, March 9). Expanding postpartum Medicaid
Coverage. Kaiser Family Foundation. https://www.kff.org/womes-health-policy/issue-brief/expanding-postpartum-
medicaid-coverage/view/.
Rayburn, W. F. (2017). The obstetrician-gynecologist workforce in the United States: Facts,
figures, and implications. The American Congress of Obstetricians and Gynecologists.
Romano, A., James-Conterelli, S., Jennings, R., & Moran, P. (2020, October 22). Addressing the
black maternal health crisis in Connecticut through expansion of midwifery-led models of care
[PowerPoint slides]. American College of Nurse-Midwives, Connecticut Affiliate.
Strauss, N. (2018). Maximizing midwifery to achieve high-value maternity care in New York.
Choices in Childbirth.
U.S. Department of Health and Human Services. (2020). Healthy women, healthy pregnancies,
healthy futures: Action plan to improve maternal health in America.
https://aspe.hhs.gov/sites/default/files/private/aspe-files/264076/healthy-women-
healthy-pregnancies-healthy-future-action-plan_0.pdf.
Yan, J. (2020). The impact of Medicaid managed care on obstetrical care and birth outcomes:
A case study. Journal of Women’s Health, 29(2), 167-176. https://doi.org/10.1089/jwh.20...